Indocyanine Green (ICG) in Bariatric Surgery
April 28, 2025
The Problem: Undetected Staple Line Leaks in Bariatric Surgery.
A small leak can lead to major complications in bariatric surgery. Staple line leaks are among the most feared complications in procedures like sleeve gastrectomy and gastric bypass. These leaks can result in infections, sepsis, prolonged hospital stays, reoperations, and even death.
Early detection is critical—and Indocyanine Green (ICG) fluorescence imaging is quickly becoming a trusted tool for intraoperative leak testing.
What Is ICG and Why Does It Matter?
Indocyanine Green (ICG) is a water-soluble dye first introduced to medicine in 1957. When exposed to near-infrared (NIR) light, ICG fluoresces, enabling real-time visualization of perfusion and leakage. Historically used in liver function, cardiac imaging, and ophthalmology, its use has expanded into surgery—particularly for leak testing in gastrointestinal and bariatric procedures.
Key Benefits of ICG in Surgery:
- Provides real-time imaging under NIR light
- Detects small leaks with high sensitivity
- Does not permanently stain tissue
- Can be administered intraluminally through an orogastric tube
How ICG Leak Testing Works
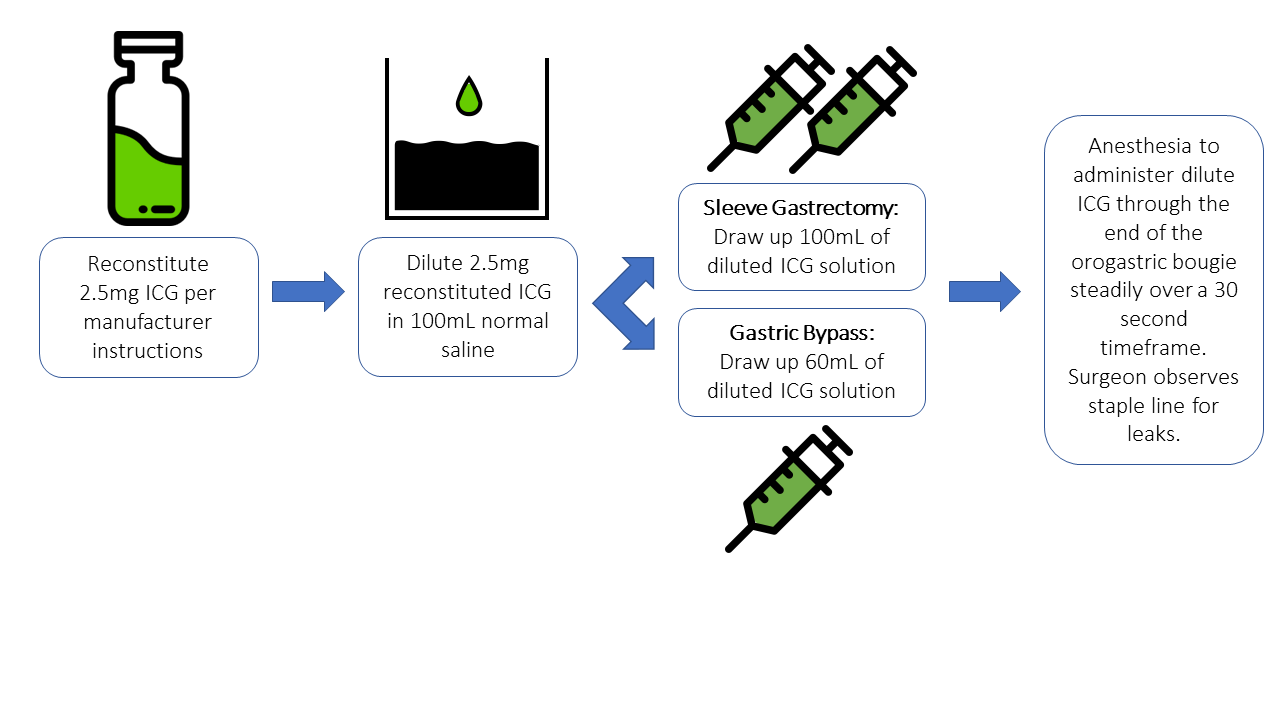
Step-by-Step Preparation and Administration
The ICG solution is reconstituted and diluted to a concentration of 2.5mg ICG per 100mL sterile saline. The anesthesiologist administers the solution through a previously placed orogastric bougie using an injectable port.
Recommended Volumes:


Real-time imaging with NIR allows the surgeon to detect fluorescence escaping from the staple line—pinpointing even minute defects before they lead to serious complications.
Visualizing the Leak: Intraoperative Imaging

Figure 1: Fluorescent ICG extravasation clearly highlights a punctate leak under NIR visualization

Figure 2: Operative field immediately after laser disengagement, showing tissue integrity
Unlike dyes such as methylene blue, ICG does not permanently stain the tissue, allowing for unobstructed repair and continued observation.
Clinical Impact: Faster, Safer Surgeries
ICG leak testing has shown value in:
- Reducing the incidence of undetected staple line leaks
- Avoiding downstream complications like enterocutaneous fistulas and sepsis
- Supporting better patient outcomes and faster recovery times
- Improving confidence for both surgeons and support staff during closure
“ICG allows for precise, visual verification of staple line integrity in real time—adding a critical safety layer to every bariatric procedure.”
Final Thoughts & Next Steps
As bariatric procedures grow in volume and complexity, safety tools like ICG fluorescence imaging are no longer optional—they’re becoming standard practice.
Interested in learning more or sourcing compatible administration tools?
Contact our clinical team or explore our surgical solutions.
References
| [1] | A. A. Alawan, J. Friedman, H. Park, R. Segal, B. A. Brumback and A. G. Hartzema, “US national trends in bariatric surgery: A decade of study,” Surgery, vol. 170, no. 1, pp. 13-17, 2021. |
| [2] | I. J. Fox and E. H. Wood, “Indocyanine green: physical and physiologic properties,” in Proceedings of the staff meetings of the Mayo Clinic, 1960. |
| [3] | J. G. Walker, H. Silva, T. R. Lawson, J. A. Ryder and S. Shaldon, “Renal blood flow in acute renal failure measured by renal arterial infusion of indocyanine green,” Experimental Biology and Medicine, vol. 11, pp. 932-5, 1963. |
| [4] | A. Wennevold and I. H. Rygg, “The interpretation of intracardiac phonocardiography of a continuous murmur developed after radical operation for tetralogy of Fallot,” Scandinavian Journal of Thoracic and Cardiovascular Surgery, vol. 2, no. 2, pp. 96-8, 1968. |
| [5] | T. A. Huffman, R. S. Goodwin, R. F. Leighton, J. M. Ryan and C. F. Wooley, “Intracarduac phonocardiography in the differential diagnosis of continuous murmus,” Annals of Internal Medicine, vol. 63, pp. 904-5, 1965. |
| [6] | K. Kogure and E. Choromokos, “Infrared absorption angiography,” Journal of Applied Physiology, vol. 26, pp. 154-7, 1969. |
| [7] | C.-H. Lu and J.-K. Hsiao, “Indocyanine green: An old drug with novel applications,” Tzu Chi Medical Journal, vol. 33, no. 4, pp. 317-322, 2021. |
| [8] | R. Gonzalez, M. G. Sarr, M. Baghai, M. Kendrick, S. Szomstein, R. Rosenthal and M. M. Murr, “Diagnosis and contemporary management of anastomotic leaks after gastric bypass for obesity,” American College of Surgeons, vol. 204, no. 1, pp. 47-55, 2007. |
| [9] | C. L. Kalmar, C. M. Reed, C. L. Peery and A. D. Salzberg, “Intraluminal indocyanine green for intraoperative staple line leak testing in bariatric surgery,” Surgical Endoscopy, vol. 34, pp. 4194-4199, 2020. |
| [10] | J. Bingham, M. Lallemand, M. Barron, J. Kuckleman, P. Carter, K. Blair and M. Martin, “Routine intraoperative leak testing for sleeve gastrectomy: is the leak test full of hot air?,” American Journal of Surgery, vol. 211, no. 5, pp. 1592-1596, 2-16. |
| [11] | G. C. Kirby, C. W. Macano, S. M. Nyasavajjala, M. Sahloul, R. Nijjar, M. Daskalakis, M. Richardson and R. Singhal, “The Birmingham experience of high-pressure methylene blue dye test during primary and revisional bariatric surgery: A retrospective cohort study,” Annals of Medicine and Surgery, vol. 23, pp. 32-34, 2017. |